

Lesley Rathbun, left, rolls a patient who needed a C-section birth to the operating room at Trident Medical Center in Charleston. (Photo provided by Lesley Rathbun/Carolina News & Reporter)
The University of South Carolina’s College of Nursing is introducing the state’s first nurse-midwifery program in Fall 2025. It will teach working nurses to be midwives in hopes of addressing the growing gap in rural maternity care that has raised concerns among healthcare experts.
“There’s poor access to care,” Jennifer Baumstark, the program director, said. “We’ve got a lot of deserts for maternity care, so hopefully we can get midwives out into those communities.”
Lesley Rathbun, a certified midwife and advocate of women’s health, said the limited access to care can no longer be ignored.
“It has got to be better because it’s going to implode,” said Rathbun, who’s from Charleston. “It’s really working quickly towards that, and we see it with the rising maternal mortality rates.”
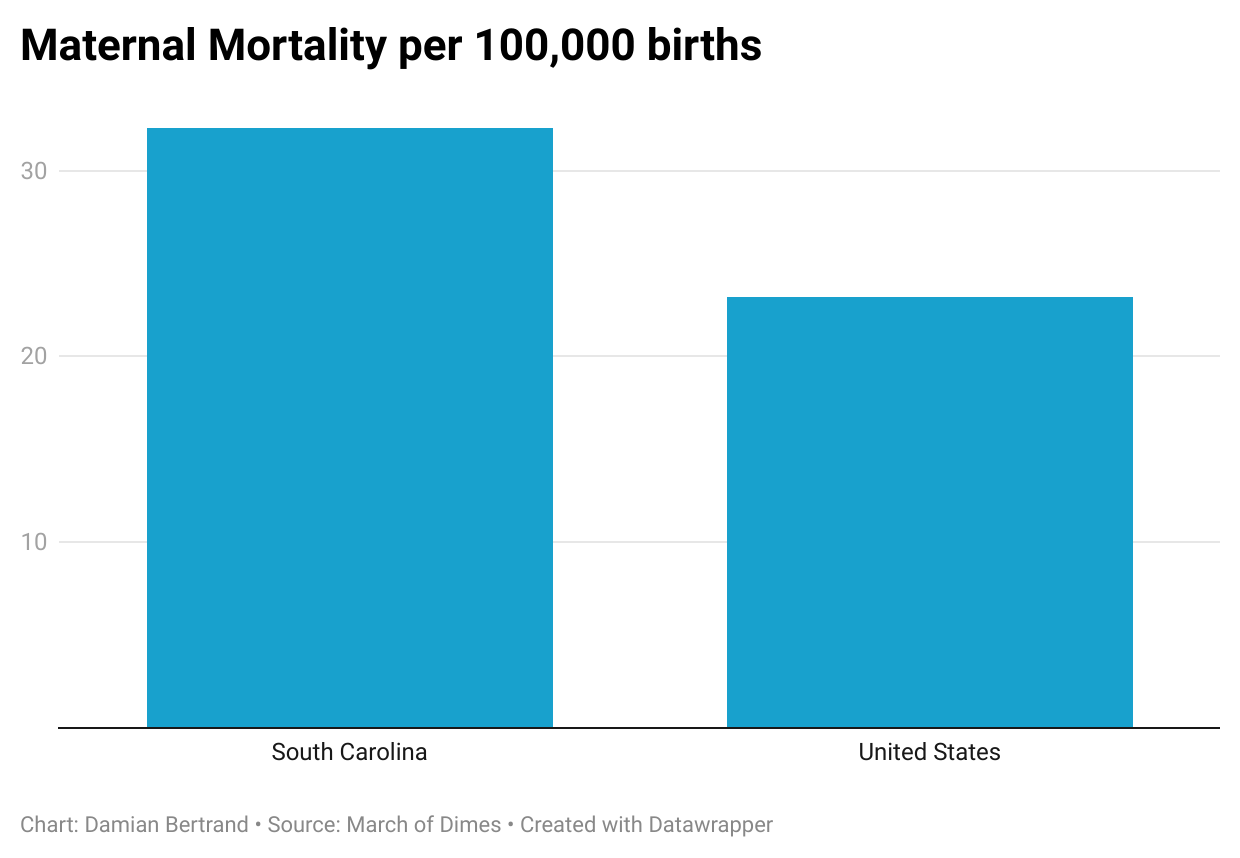
Maternal mortality in South Carolina in 2022 was 32.3 women per 100,000 births, while the United States had 23.2 deaths per 100,000 births, according to March of Dimes, a nonprofit that provides maternal and infant-health-related data.
Rural areas in South Carolina are seeing a shortage of delivery units and OB-GYNs, forcing mothers to drive to farther away hospitals.
Thirteen labor and delivery units in South Carolina have closed since 2012, according to an October report from USC’s Institute for Families in Society. That leaves mothers in rural parts of South Carolina driving longer distances or not going to the doctor at all, increasing their pregnancy-related risks.
“I was in labor, and I was about to have that baby in the back seat of the car,” said Angelica Bowling, a mother of three.
Bowling, a caregiver, lives in Hopkins and drove more than 35 minutes to Lexington Medical Center to give birth to her second child.
In South Carolina, 100% of women living in rural areas live farther than 30 minutes from the nearest birthing hospital, according to the March of Dimes.
Only 8.5% of women living in S.C. urban areas live that far from the nearest birthing hospital.
Bowling said having to drive farther gave her less time to prepare for the hospital, causing further stress on her and her family.
“I think it was more emotional than anything else,” Bowling said. “You don’t want to aggravate a pregnant woman because you get cussed out from sunup to sundown.”
Shutting down
In Columbia, Providence Health-Northeast could have been an option for Bowling, she said.
But it had to eliminate its obstetrical services because it wasn’t profitable, said Dr. Douglas Addy, an OB-GYN at Lexington Medical Center. It’s now owned by the Medical University of South Carolina.
“Obstetrical services don’t make a lot of money, especially on a small scale, and the government doesn’t pay well,” Addy said. “It’s just the nature of healthcare.”
That is true for most delivery units in rural South Carolina, Rathbun said.
Rathbun is a past president of the American Association of Birth Centers, an organization that supports birth centers and encourages the growth of midwives, nurses with advanced training who specialize in women’s reproductive health and childbirth.
“Maternity care tends to be a loss-leader for corporations that own and operate hospitals,” Rathbun said. “The cost of care is increasing rapidly. But the reimbursement for that care has been decreasing.”
The payment rate for obstetrics is lower than in the 1990s, leading to fewer nurse midwives and obstetricians, Rathbun said.
“They also burn out quickly,” Rathbun said. “The years worked for a nurse midwife over a career is much less than if you compare it to some higher-paid medical professions, like orthopedics and cardiology.”
Fewer obstetricians lead to more delivery unit closures.
The MUSC Health Kershaw Medical Center in Camden had a delivery unit but removed it last year because there weren’t enough babies being delivered to offset the operations cost, MUSC said at the time.
Kershaw County women now drive an extra 30 minutes to MUSC Health Columbia Medical Center Northeast, the next closest delivery unit.
“Camden people have nowhere to go, at least locally,” Addy said. “I’m sure the hospital wanted to maintain and develop their obstetrical abilities. But if it doesn’t pay well, no one’s going to be able to maintain it.”
The Risks
In 2023, six of South Carolina’s 46 counties were labeled “maternity care deserts,” where women have no access to OB-GYNs or midwives, according to a March of Dimes report.
That number is increasing, said Deborah Hopla, a professor and director of the nurse practitioner program at Francis Marion University in Florence.
Fifteen counties have zero OB-GYNs per 10,000 women, and 28 counties have zero midwives per 10,000 women to help with deliveries, according to a 2024 report from the South Carolina Office for Healthcare Workforce.
Nearly 40% of counties in South Carolina have women living with a very high or high vulnerability to adverse outcomes, such as preterm birth, depression and maternal mortality. The vulnerability is due to the unavailability of reproductive healthcare services, according to March of Dimes.
Women who live further away from obstetrical services are less likely to receive prenatal care, which is vital to reduce maternal mortality, Hopla said.
“A lot of women are still not getting prenatal care, and so then you’re having babies that are born that haven’t had prenatal care,” Hopla said. “They just show up to have their baby delivered, and then they have bad outcomes.”
South Carolina ranks 8th in the nation in maternal mortality, according to a 2024 report from the South Carolina Maternal Morbidity and Mortality Review Committee.
“That means more women die here than just about anywhere except Mississippi,” Hopla said. “But what a terrible thing to say, ‘Come here and your mothers and babies will die.’”
What needs to be done
It’s a matter of money to stop the shortage of OB-GYNs in rural areas, Addy said.
But even then, there are more obstacles for upcoming nurses and doctors.
“You can make it more financially available, but there’s a big shortage of doctors coming, and doctors have kind of done that to themselves, with the increase of medical education tuition,” Addy said. “It’s crazy how hard it is to get into med school.”
That’s where midwives become all the more important.
Birthing centers, maternal care facilities led by midwives, outperform hospitals when it comes to effectiveness and cost saving, Rathbun said. But they need more money, she said.
“The entire healthcare system needs to recognize that maternity care is important,” she said. “We know without a doubt that this is the model that works.”
Francis Marion’s Hopla still has hope that USC’s nurse-midwifery program will increase maternity care access in the future.
And she wanted to help.
So she raised money through the South Carolina Health Action Coalition, an organization that runs on grant money from national philanthropic groups and aims to reduce maternal and infant mortality rates.
A key goal is to help increase the percentage of midwives in the state, Hopla said.

A labor and delivery room at Lexington Medical Center (Photo courtesy of Lexington Medical Center/Carolina News & Reporter)

Lesley Rathbun shampoos a baby she had recently delivered. (Photo provided by Lesley Rathbun/Carolina News & Reporter)

Deborah Hopla, a nurse practitioner at HopeHealth Medical Plaza in Florence (Photo courtesy of Deborah Hopla/Carolina News & Reporter)

{kind=link}